In recent years the most popular isokinetic test in the shoulder has been internal/ externalrotation (with modified seated in the scapular plane being the most popular). The main reason this test has become so popular is the open chain nature of shoulder motions. Most movements around the shoulder in everyday life, and in fact sport, occur with the hand free in space (open chain). The position of the shoulder joint (humeral head in the glenoid fossa) is actually controlled by a small group of muscles know collectively as the rotator cuff. This group is referred to as a cuff as they make up a significant portion of the front of the shoulder joint capsule (anterior joint capsule or sulcus).
The rotator cuff muscles (supraspinatous, infraspinatous, teres minor and subscapularis) control the position of rotation of the arm in space and they also locate the humeral head in the glenoid fossa. If the rotator cuff is not functioning correctly then pain and dysfunction usually follows.
Many sports will involve training one (or several) muscles of the rotator cuff preferentially. This can lead to muscle imbalance across the shoulder which in turn affects the position of the shoulder (shoulder posture) and can lead to pain and impingement. Overuse of the muscles (and particularly tendons) can lead to tears in either the muscle, tendon /s or the joint capsule (as the tendons constitute a large portion of the anterior capsule).
The two main problems at the front of the shoulder (know as anterior shoulder pain) can be assessed and in fact prevented using isokinetic testing and exercise:
Impingement: normally caused by altered muscle balance and altered activation of muscles (testing of supraspinatous and infraspinatous 80-90% accurate according to Hegedus et al. 2008).
Tear: either tendon or muscle (can be tendinitis or capsulitis) are seen in the strength difference between sides and the shape of the MAP curve.
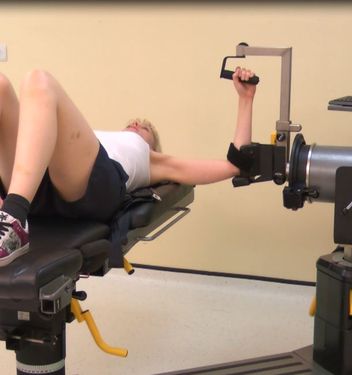
Lying position (90 degrees abduction):
The most stabilised position for testing rotation and offers the greatest range of motion. However it takes the shoulder into it’s most vulnerable position (known as the closed pack position which is 90 degrees abduction with full external rotation). Use of this position more specifically addresses the muscular function required for overhead throwing activities (Bassett et al. 1994). Best for research but do not use with patient populations.
To view a set up video see below:
Seated position:
There are 2 main positions for testing shoulder rotation in the seated position they are:
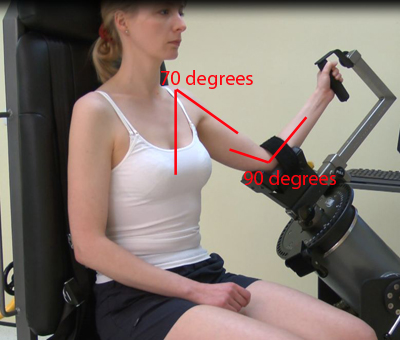
Modified Seated:
The most popular position as it allows control of the position of the scapular (this allows the scapular plane to be used). Although this position is not as stabilised and does not allow as large a range of motion it is functional and gives the most usable results. Best for patients.
This position has been termed the 30/30/30 position by Davies (1992). The subjects gleno-humeral joint is placed in 30 degrees abduction (this has been changed in more recent studies) 30 degrees forward flexion (scaption) and 30 degrees upward tilt of the dynomometer. This places the shoulder in the scapular plane 30 degrees anterior to the coronalplane. As the shoulder is in the scapular plane there is enhanced bony congruity and a neutral glenohumeroal position (Ellenbecker and Davies 2000). In turn this leads to a mid-range position for the anterior joint capsular ligaments (rotator cuff) and enhances the muscular efficiency of the rotator cuff. Most importantly it does not place the suprahumeral structures in a vulnerable position (it limits impingement) according to Saha (1971).
Ellenbecker and Davies 2000 reported the test retest reliabilty of this position at speeds of 60, 180 and 300 degrees per second and found intraclass correlation coefficients ranging between 0.91 and 0.96 making the position very reliable.
One of the main reasons this position has been focused on is because of work done by Quincy et al. (2000). They found that after 6 weeks of training in this position there were significant improvments in strength in all motions. That included flexion, extension, abduction, adduction and both rotations. This overflow of strength is a key factor in it’s choice in rehabilitation.
The position of the scapula needs to be set before the movements take place. A scapula angle of 20-30 degrees (see below) should be used (the scapular plane) as this offers the best alignment for the rotations to occur around with minimal scapula involvement.

The next consideration is the height of the shoulder gridle. Most authors recommend neutralas the optimal position be guided by subject comfort try to avoid elevation or depression (see below)

Some clinicians use a spirit level to align the humerous to level with the floor but the prefered position is somewhere near 70-75 degrees abduction (remember consistency is the key!). The elbow should be flexed to 90 degrees (see below).
Once the position of the scapula and gleno-humeraljoint neutral has been reached then the actuator should already be co-linear with that of the humerus through the olecranon (Wilk et al. 1991). Or in other words once you have the subject in place the elbow will be opposite the actuator axis as the designers have made it that way. Stabilization is achieved with thoracic strapping.
To view a set up video see below:
Seated 90 degrees flexion:
The less popular seated position as it linits the position of the scapular (placing it in almost full protraction). This position is more stabilised than modified seated, however, it does not allow much range of motion at all as the legs limit the internal rotation.
The position of the scapula and shoulder are set by lifting the arm to 90 degrees and protracting the scapular.

Once the position of the scapula and gleno-humeral joint have been reached then the actuator should already be co-linear with that of the humerus through the olecranon (Wilk et al. 1991). Or in other words once you have the subject in place the elbow will be opposite the actuator axis as the designers have made it that way. Stabilization is achieved with thoracic strapping.
To view a set up video see below:
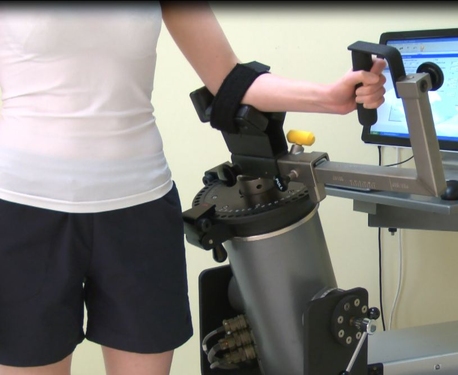
Standing position:
In the standing position (see below) stabilization is difficult if not impossible (and probably undesirable). Testing in this position is more functional than that in any other position expect corelation coefficients to be as low as 0.71.
To view a set up video see below:
Stabilisation:
Lying: In the lying position stabilisation normally only involves a pelvic strap to prevent the torso from influencing the results.
Standing: Stabilistion in the standing position is not normally required as this is the most functional position.
Seated: in the seated position stabilisation usually involves chest straps and an elbow strap.
Attachments:
There is validity in using a wrist strap (as seen in modified seated middle picture above) rather than a grip handle (as seen in standingabove) because this eliminates the influence of the wrist flexors and extensors. Although this may have some face validity it does not translate into real world testing. The hand grip is then always preferable.
Axis of rotation:
Once the position of the scapula and gleno-humeral joint have been reached then the actuator should already be co-linear with that of the humerus through the olecranon (Wilk et al. 1991). Or in other words once you have the subject in place the elbow will be opposite the actuator axis as the designers have made the elbow support that way.
Anatomical zero:
Mid way between internal and external rotation (a small magnetic spirit level is useful here it can be used to show 90 degrees, parallel to the floor and 45 degree angle for consistency.
Range of motion:
Generally a large range of motion is chosen for these tests. The test is often limited to the amount available before the arm hits a body part or the chair. However in standing and lying the range is unlimited.
Although it may be possible to go to extreme external rotation (some baseball pitchers have 180 degrees + from anatomical zero) it is not normally tested beyond 90 degrees. Internal rotation of up to 180 degrees can be produced but once again anything below 90 degrees is normally used.
Gravity correction:
As the lever arm can be very long and heavy in these movements setting of gravity correction is essential. In patients gravity elimination (HumacNorm) can be very beneficial to reduce ballistic forces.
Speeds:
As velocities in some sports (any involving throwing an object) are known to reach thousands of degrees/second (Pappas et al., 1985) testing using a dynamometer been said to be non-functional. However, speeds over 300 degrees/second have been found to be difficult to achieve by even baseball pitchers (Cook et al., 1987). This could be said to suggest that muscular effort starts the motion but only occurs at slower speeds with momentum and acceleration playing a larger role later in the speed of the motion later through range rather than pure strength. Even if this speed could be achieved it is over such a small arc that the results gained would likely be fruitless.
Generally it is accepted that speeds of 60 degrees/second and multiples of this should be used.
Shoulder Internal / External Rotation Protocols:
Muscles involved:
Subscapularis, infraspinatus, supraspinatus, teres minor, latissimus dorsi and pectoralis major
| Strength Test Protocols | General | Patients | Athletes | Research |
| Contraction Cycle | con/con | con/con | con/concon/ecc | con/conecc/ecc |
| Speed/s | 60 or 120 | 60 or 120 | 60-300 | 60-500 |
| Trial Repetitions | 0 | 0 | 0 | 3 |
| Repetitions | 10 | 10 | 10 | 5 |
| Sets | 3 | 3 | 4 | up to 9 |
| Rest between sets | 20-30 secs | 20-30 secs | 20-30 secs | 20 secs |
| Rest between speeds | 2 minutes | 2 minutes | 2 minutes | 2-5 minutes |
| Rest between sides | 5 minutes | 5 minutes | 5 minutes | 5 minutes |
| Feedback | nil | nil | nil | nil |
| Endurance Test Protocols | General | Patients | Athletes | Research |
| Contraction Cycle | con/con | con/con | con/concon/ecc | con/conecc/ecc |
| Speed/s | 120 | 120 | 120-300 | 120-500 |
| Trial Repetitions | 0 | 0 | 0 | 0 |
| Repetitions | Max | Max | Max | Max |
| Sets | 1 | 1 | 1 | 1 |
| Rest between sets | N\A | N/A | N/A | N/A |
| Rest between speeds | 10-15 mins | 10-15 mins | 10-15 mins | 10-30 mins |
| Rest between sides | 5 mins | 5 mins | 5 mins | 5 mins |
| Feedback | nil | nil | nil | nil |
| Strength Exercise Protocol | General | Patients | Athletes |
| Contraction Cycle | con/con | con/con | con/ecc |
| Speed/s | 60 up to 180 | 60 up to 180 | 60-300 |
| Trial Repetitions | 0 | 0 | 0 |
| Repetitions | 10 | 10 | 14 |
| Sets | 6 | 6 | up to 12 |
| Rest between sets | 30-60 secs | 30-60 secs | 30 secs |
| Rest between speeds | 2 mins | 2 mins | 2 mins |
| Rest between sides | Nil | Nil | Nil |
| Feedback | bar | bar | bar |
| Endurance Exercise Protocol | General | Patients | Athletes |
| Contraction Cycle | con/con | con/con | con/con |
| Speed/s | 120-180 | 120-180 | 120-300 |
| Trial Repetitions | 0 | 0 | 0 |
| Repetitions | Max | Max | Max |
| Sets | 1-3 | 1 | 1-3 |
| Rest between sets | 5-10 mins | N/A | 5-10 mins |
| Rest between speeds | 10-30 mins | N/A | 10-30 mins |
| Rest between sides | Nil | Nil | Nil |
| Feedback | bar/pie chart | bar/pie chart | bar/pie chart |
Notes:
Test the uninvolved or dominant limb first.
Interpretation:
In the shoulder it is normal to look at the ratio between the right and left sides there should be a 0-10% difference between the sides. Anything beyond this would either demonstrate extreme hand dominance (this can happen in certain sports like javelin), or indicate a muscle imbalance which would be best corrected.
Eccentric results are generally 34% higher than concentric within the same muscle Ivey et al (1985) Davies (1984).
In rotations it is also common to look at muscle balance across the joint. Internalrotation is normally stronger than external rotation by 30-40% (Brown 2000). It is also possible to compare concentric to eccentric results across the joint this normally involves looking at concentric internalrotation compared to eccentric external rotation. In throwing sports the concentric internalrotation is used to accelerate the throw and then the eccentric external rotators are used to slow the shoulder to a stop. So it is common to look at the ratio between concentric internalrotation and eccentric external rotation. The stronger the eccentric action the better the result. On some dynamometers(Norm) the angle of the torque production can be analysed. This is important in this equation as the angle of peak torque of the eccentric external rotation may not be the same as the concentric internal rotation (this can sqewthe results usually in favour of the external rotators). If this facility is available use the @angle function to check the torque of the eccentric action to the angle of peak torque in the concentric action.
Supraspinatous Tendonitis:
The torque curve is usually flattened during the concentric phase of either internal or external rotation (dependent on the position of the humorous).
If the test is performed in 90 degrees of abduction (lying position) then the curve will be flattened in the latter half of internal rotation see next figure.
If the test is performed in any other position the curve will be flattened in the external rotation component see next figure.
Subscapularis Tendonitis:
The torque curve is similar to that seen in shoulder impingement, however, a normal curve is usually seen in early repetitions with changes only evident in later repetitions.
This is probably due to a gradual build up of pain during the test.
Graph shown for internal rotation modified seated.
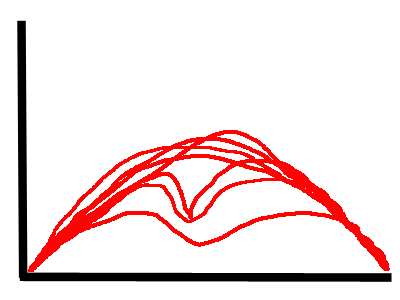
Note the graph shown is a curve overlay graph.
Normative values:
| Wilk et al. (1993) | Age | Sex | Machine | Nm mean (SD) | Nm mean (SD) |
| speed deg/s | Internal Rot | External Rot | |||
| 180 Non Dominant | 52.4 (9.5) | 36.5 (6.8) | |||
| 300 | 30.1 (6.3) | ||||
| 180 Dominant | 53.9 (8.8) | 34.5 (6.2) | |||
| 300 | 29.3 (5.1) | ||||
| Alderink & Kuck (1986) | PTBW | PTBW | |||
| 90 | 22 | 15 | |||
| 120 | 15 | ||||
| 210 | 19 | 14 | |||
| 300 | 13 | ||||
| Chandler et al. (1992) | ftlbs | ftlbs | |||
| 60 | |||||
| 300 | |||||
| PTBW | PTBW | ||||
| 60 | |||||
| 300 | |||||
| IR/ER Ratio | IR/ER Ratio | ||||
| 60 | |||||
| 300 | |||||
| Ellenbecker & Mattalino | IR/ER % Dominant | IR/ER % Non Dom | |||
| 210 PT | 64 | 74 | |||
| 210 Work single rep | 61 | 66 | |||
| 300 PT | 65 | 72 | |||
| 300 Work single rep | 62 | 70 | |||
| Wilk et al. | |||||
| 180 PT | 65 | 64 | |||
| 300PT | 61 | 70 | |||
| Biodex Values | N/A | M | Biodex | PTBW Goal | PTBW Goal |
| 60 mod seated | 19-26 | 14-18 | |||
| 180 | 17-23 | 13-17 | |||
| F | |||||
| 60 | 13-17 | 10-13 | |||
| 180 | 11-15 | 8-12 |
| Ellenbecker & Davies (2000) | Dominant Arm | Non Dominant Arm | ||
| Motion & Speed | Peak torque % | Work% | Peak torque% | Work% |
| External Rotation | ||||
| Male 210 | 12 | 20 | 11 | 19 |
| Male 300 | 10 | 18 | 10 | 17 |
| Female 210 | 8 | 14 | 8 | 15 |
| Female 300 | 8 | 11 | 7 | 1 |
| Internal Rotation | ||||
| Male 210 | 17 | 32 | 14 | 27 |
| Male 300 | 15 | 28 | 13 | 23 |
| Female 210 | 12 | 23 | 11 | 19 |
| Female 300 | 11 | 15 | 10 | 13 |
| ER/IR ratio% | ||||
| Male 210 | 51 | 64 | 80 | 78 |
| Male 300 | 70 | 65 | 81 | 80 |
| Female 210 | 70 | 66 | 79 | 82 |
| Female 300 | 67 | 69 | 77 | 80 |
Values for internal rotator group concentric and eccentric strength (in Nm). Based on Ivey et al (1985), Cahalan et al (1991) and + Shkiar & Dvir (1994) sedentary subjects.
| 600/s | 1200/sec | 1800/sec | 3000/sec | |
| Concentric | ||||
| Men | 55 | 40 | 49 | 42 |
| Women | 28 | 26 | 23 | 22 |
| Eccentric | ||||
| Men | 47 | 45 | ||
| Women | 26 | 26 |
Values for shoulder external rotation group concentric and eccentric strength (in Nm). Based on Ivey et al (1985), Cahalan et al (1991) and + Shkiar & Dvir (1994) sedentary subjects.
| 600/s | 1200/sec | 1800/sec | 3000/sec | |
| Concentric | ||||
| Men | 33 | 23 | 27 | 20 |
| Women | 19 | 15 | 13 | 9 |
| Eccentric | ||||
| Men | 31 | 31 | ||
| Women | 19 | 19 |
Hughes et al (1999) looked at shoulder internal/external ratios between the dominant and non dominant sides:
| angle of abduction | Dominant Side % (sd) | Non Dominant Side % (sd) | Average % |
| 0 | 0.58 (0.14) | 0.62 (0.24) | 0.60 (0.16) |
| 90 | 0.75 (0.23) | 0.70 (0.22) | 0.73 (0.19) |