In recent years the use of hip testing both isokinetic and isometric testing has been on the increase.
The main areas the research has seemed to focus on are:
Femoroacetabular Impingement (FAI)
Brunner et al. 2016
Diamond, Wrigley, Hinman 2015
Casartelli et al1. 2014
Casartelli et al2. 2012
Hip muscle function has been said to be altered in patients with FAI. Casartelli et al. (2012) described decreased isometric muscle strength (tested on an isokinetics machine) of the hip flexors, adductors, abductors and external rotators compared with controls. However, Diamond et al. (2015) only found 20% lower isometric abduction strength in FAI than controls (p = 0.04). With no significant differences in isometric strength for other muscle groups or peak isokinetic ER or IR strength. They did find the ratio of isometric, but not isokinetic, ER/IR strength was significantly higher in the FAI group (p = 0.01). But again there were no differences in the other ratios. The only really telling factor was angle of peak IR torque isokinetically which correlated with symptoms. Brunner et al. (2016) did not find significant isokinetic differences in hockey players with FAI. The study was of both symptomatic and asymptomatic players meaning isokinetic testing may not be a good diagnostic tool in this injury.
Falls and Hip Replacements
Morcelli et al. 2016
Melchiorri et al 2015
Rogers 2015
Normative Values
Bittencourt et al. 2016 (basketball, hockey, futsal or 5 a side soccer)
Brent et al. 2013 (male to female values in soccer and basketball)
Harbo , Brincks, and Andersen 2012 (normative values in population)
Positioning:
These movements can be performed in either the lying (supine), or seated (modified) positions.
The hip has the same degrees of freedom (movements) as the shoulder, however, unlike the shoulder the hip is bound tightly to the pelvic girdle making it much more stable. This stability gives the hip virtually no intrinsic motion. This limits the hips motion in each plane. This stable configuration reduces the possible contraindications and compensations (pelvic anterior / posterior rotation in hip rotation testing) are limited and easily identifiable. The bony landmarks are easy to find and the range of motion can be used without limitation as injury is unlikely.
The actions of the hip muscles are complex and often change in relation to demands. Any functional motion requires a coordinated effort by several muscles which may participate in many different actions together or individually. The function of some muscles (Medial gluteal is a good example as the posterior section rotates the hip inwards whilst the anterior section can rotate it outwards) changes depending on hip position and whether the position is weight bearing or not.
Lying position:
The least stabilised position for testing rotation.

To view a set up video see below:
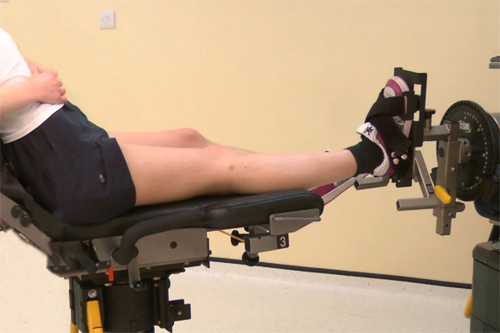
Seated position:
The position of choice for patients and research (Lindsay et al. 1992). To modify the position simply sit the back of the chair up to the 70 degree angle.
Hip Flexion Angle:
Baldon, Furlan, and Serrão (2013) looked at hip rotator function at 3 different hip flexion angles (10°, 40°, and 90°).
The results showed that both eccentric and concentric hip lateral rotator torques were greater at 40° of hip flexion when compared with 90°. However, both the eccentric and concentric hip medial rotator torques were greater at 90° of hip flexion than at 40° (and 10°), but 40° was still higher than 10°.
In addition, both the eccentric and concentric hip medial to lateral rotator torque ratios were greater at 90° of hip flexion than at 40° (40° was still higher than at 10°).
Finally, the acceleration times of the hip medial rotator muscles were smaller at 90° of hip flexion than at 10° and smaller at 40° than at 10°.
So if your only interested in lateral rotation use 40 degrees hip flexion (if you were doing con/ecc lateral/external rotation)
But if you are testing medial rotation (con/ecc) or medial and lateral rotation (con/con) use 90 degrees. This includes getting a lat/med or int/ext rot ratio
The only time to use 10 degrees is in acceleration testing.
IF IN DOUBT USE 90 degrees!!!
Stabilisation:
Lying: In the lying position stabilisation normally only involves a pelvic strap to prevent the torso from influencing the results and a leg strap for the opposite (non tested) leg.
Seated: Stabilisation normally only involves a pelvic strap to prevent the torso from influencing the results
Attachments:
The footplate is normally used.
Axis of rotation:
The instantaneous axis of rotation is simply along the long axis of the femur
Anatomical zero:
With foot pointing to roof.
Range of motion:
Although the hip has equal ROM to internal/external rotation of 45 degrees (Miller, 1985) isokinetic testing of these movements can be done over a much shorter arc.
Dvir (1995) suggests a ROM from 5 degrees internal rotation to 25 degrees of external rotation.
Be careful not to overstress the joint capsule in these tests.
Gravity correction:
Can be carried out if required but the influence is small some manufacturers supply a counter balance to use instead.
Speeds:
It seems currently the lowest velocity used is 60 deg/sec.
In studies looking at hip strength and knee pain 120 deg/sec is most popular.
Authors like Mohammad (2015) have been up as high as 180 deg/sec with no patient compliance issues or dynamometer problems (it must be noted higher speeds should only be used on a Norm 2009 on or a Biodex system 3 on).
Hip Internal / External Rotation Protocols:
Muscles involved:
Obturators and Gluteals
| Strength Test Protocols | General | Patients | Athletes | Research |
| Contraction Cycle | con/con | con/con | con/concon/ecc | con/conecc/ecc |
| Speed/s | 60 or 120 | 120 | 30-300 | 30-500 |
| Trial Repetitions | 0 | 0 | 0 | 3 |
| Repetitions | 10 | 10 | 10 | 5 |
| Sets | 3 | 3 | 4 | up to 9 |
| Rest between sets | 20-30 secs | 20-30 secs | 20-30 secs | 20 secs |
| Rest between speeds | 2 minutes | 2 minutes | 2 minutes | 2-5 minutes |
| Rest between sides | 5 minutes | 5 minutes | 5 minutes | 5 minutes |
| Feedback | nil | nil | nil | nil |
| Endurance Test Protocols | General | Patients | Athletes | Research |
| Contraction Cycle | con/con | con/con | con/concon/ecc | con/conecc/ecc |
| Speed/s | 120 | 120 | 60-300 | 60-500 |
| Trial Repetitions | 0 | 0 | 0 | 0 |
| Repetitions | Max | Max | Max | Max |
| Sets | 1 | 1 | 1 | 1 |
| Rest between sets | N\A | N/A | N/A | N/A |
| Rest between speeds | 10-15 mins | 10-15 mins | 10-15 mins | 10-30 mins |
| Rest between sides | 5 mins | 5 mins | 5 mins | 5 mins |
| Feedback | nil | nil | nil | nil |
| Strength Exercise Protocol | General | Patients | Athletes |
| Contraction Cycle | con/con | con/con | con/ecc |
| Speed/s | 60 120 | 120 | 30-300 |
| Trial Repetitions | 0 | 0 | 0 |
| Repetitions | 10 | 10 | 14 |
| Sets | 6 | 6 | up to 12 |
| Rest between sets | 30-60 secs | 30-60 secs | 30 secs |
| Rest between speeds | 2 mins | 2 mins | 2 mins |
| Rest between sides | Nil | Nil | Nil |
| Feedback | bar | bar | bar |
| Endurance Exercise Protocol | General | Patients | Athletes |
| Contraction Cycle | con/con | con/con | con/con |
| Speed/s | 60-120 | 60-120 | 60-300 |
| Trial Repetitions | 0 | 0 | 0 |
| Repetitions | Max | Max | Max |
| Sets | 1-3 | 1 | 1-3 |
| Rest between sets | 5-10 mins | N/A | 5-10 mins |
| Rest between speeds | 10-30 mins | N/A | 10-30 mins |
| Rest between sides | Nil | Nil | Nil |
| Feedback | bar/pie chart | bar/pie chart | bar/pie chart |
Notes:
Test the uninvolved or dominant limb first.
Interpretation:
In the hip it is normal to look at the ratio between the right and left sides there should be a 0-10% difference between the sides. Anything beyond this would indicate a muscle imbalance which would be best corrected.
Eccentric results are generally 30% higher than concentric within the same muscle.
Concentric/concentric ratio; external/internal rotation 0.80% this means the external rotators are only 80% of the extensors or the other way around is the internal rotators are 20% stronger than the external rotators
Normative values:
| Tippett (1986) | sex | age | Internal | External |
| M | 20 | |||
| 30 dominant | 30 | 25 | ||
| 30 non dominant | 30 | 26 | ||
| 180 dominant | 17 | 16 | ||
| 180 non dominant | 16 | 13 |
Hip internal and external rotator concentric strength (based on Cahalan et al 1989 and Lindsey et al 1992)
| Female | Male |
| 18-30 yrs. | 20-40 yrs. | 40-81 yrs. | 18-30 yrs. | 20-40 yrs. | 40-81 yrs. | |
| Internal | ||||||
| 30/sec | 40 | 34 | 72 | 61 | ||
| 60/sec | 86 | 139 | ||||
| 90/sec | 36 | 22 | 53 | 41 | ||
| External | ||||||
| 30/sec | 43 | 32 | 65 | 50 | ||
| 60/sec | 53 | 84 | ||||
| 90/sec | 31 | 21 | 49 | 38 |