Another test rising in popularity due to FAI and falls.
Femoroacetabular Impingement (FAI):
Hip muscle function has been said to be altered in patients with FAI. Casartelli et al. (2012) described decreased isometric muscle strength (tested using an isokinetics machine) of the adductors and abductors compared with controls.
However, Diamond et al. (2015) only found 20% lower isometric abduction strength in FAI than controls (p = 0.04). With no significant differences in isometric strength for other muscle groups.
Falls:
Rogers (2015) said younger adults engage a single more stable loaded-limb sidestep. This is achieved by actively unloading and advancing the limb.
Older adults use less stabilizing and hence more precarious multiple unloaded limb crossover and medial steps.
These differences in first-step recovery patterns appear to involve ageing decrements in hip AB-AD joint torque and power production.
Collectively, the use of multiple recovery steps during lateral perturbation trials, reduced maximum isokinetic hip Abd torque, and led to shorter global first step length. This reduction, Rogers (2015) postulated, could significantly predict future falls among older adults.
Positioning:
Although the position is referred to abduction and adduction because of the soft tissue opposition (one leg hits the other) the motion of adduction is normally described from abduction back to neutral (in lying) or slightly beyond (in standing).
These movements can be performed in either the lying (side or supine), or standing positions.
The hip has the same degrees of freedom (movements) as the shoulder, however, unlike the shoulder the hip is bound tightly to the pelvic girdle making it much more stable. This stability gives the hip virtually no intrinsic motion. This limits the hips motion in each plane. This stable configuration reduces the possible contraindications and compensations (anterior tilt in abduction) are limited and easily identifiable. The bony landmarks are easy to find and the range of motion can be used without limitation as injury is unlikely.
The actions of the hip muscles are complex and often change in relation to demands. Any functional motion requires a coordinated effort by several muscles which may participate in many different actions together or individually. The function of some muscles (Medial gluteal is a good example as the posterior section rotates the hip inwards whilst the anterior section can rotate it outwards) changes depending on hip position and whether the position is weight bearing or not.
Lying position (side):
The most stabilised position for testing abduction but it limits adduction to the neutral position. Best for abduction research poor for adduction.

To view a set up video see below:
Lying position (supine):
This position requires a dynomometer with allot of height adjustment (Kin-Com) it can be difficult to stabilise correctly.

Standing position:
In the standing position (see below) stabilisation is difficult if not impossible (and probably undesirable). Testing in this position is more functional than that in the seated position and allows the investigation of adduction. It is claimed that this is more functional and involves the use of gravity. Flexion of the knee is recommended, although only passively against gravity if for no other reason than to avoid sciatic nerve traction. Testing in in the upright position is more in line with the use of the limb in the real world. In real life most adduction movements occur either in front of, or behind, the mid line which can be achieved in the standing position. Mohammad (2015) found high reliability measures when comparing standing to the side lying position. Best for athletes.

To view a set up video see below
Stabilisation:
Lying: In the lying position stabilisation normally only involves a pelvic strap to prevent the torso from influencing the results and a leg strap for the opposite (non tested) leg.
Standing: Stabilisation in the standing position is not normally required as this is the most functional position.
Attachments:
Lying (side) and Standing: The thigh stabiliser pad is normally used and should be positioned just proximal to the knee joint.
Supine: The pad should be placed just above the foot to hold the weight of the limb. A dual pad can be obtained as described by Donatelli et al. (1991) however this is not necessary. (The knee must be kept straight during the test.)
Axis of rotation:
The instantaneous axis of rotation place the actuator axes opposite the hip joint 1 cm medially to the anterior superior iliac spine (red line seen above).
Anatomical zero:
With leg straight (as in standing).
Range of motion:
The accepted ROM for abduction is 45 degrees whereas for adduction it may be up to 25 degrees (Miller, 1985). Obviously movements into adduction are usually prevented by a mechanical block (the other leg).
Gravity correction:
As the lever arm can be very long and heavy in these movements setting of gravity correction is essential.
Speeds:
Donatelli et al. (1991) suggest velocities between 30-90 degrees/second, however, These would now be considered to be too low.
Dos Santos Andrade et al. (2015) found ICC for peak torque in abduction and adduction ranging from 0.55 to 0.76 (high reliability) at 150º/s. These were once again higher than the results at 30º/s
And again Mohammad (2015) found higher correlations at 180º/s than the tests at 60º/s
If in doubt go faster not slower.
Hip Abduction / Adduction Protocols:
Muscles involved:
Gluteals, tensor fascia late and adductor group
| Strength Test Protocols | General | Patients | Athletes | Research |
| Contraction Cycle | con/con | con/con | con/concon/ecc | con/conecc/ecc |
| Speed/s | 30 up to 180 | 30 up to 180 | 30-300 | 30-500 |
| Trial Repetitions | 0 | 0 | 0 | 3 |
| Repetitions | 10 | 10 | 10 | 5 |
| Sets | 3 | 3 | 4 | up to 9 |
| Rest between sets | 20-30 secs | 20-30 secs | 20-30 secs | 20 secs |
| Rest between speeds | 2 minutes | 2 minutes | 2 minutes | 2-5 minutes |
| Rest between sides | 5 minutes | 5 minutes | 5 minutes | 5 minutes |
| Feedback | nil | nil | nil | nil |
| Endurance Test Protocols | General | Patients | Athletes | Research |
| Contraction Cycle | con/con | con/con | con/concon/ecc | con/conecc/ecc |
| Speed/s | 90 | 60 | 90-300 | 90-500 |
| Trial Repetitions | 0 | 0 | 0 | 0 |
| Repetitions | Max | Max | Max | Max |
| Sets | 1 | 1 | 1 | 1 |
| Rest between sets | N\A | N/A | N/A | N/A |
| Rest between speeds | 10-15 mins | 10-15 mins | 10-15 mins | 10-30 mins |
| Rest between sides | 5 mins | 5 mins | 5 mins | 5 mins |
| Feedback | nil | nil | nil | nil |
| Strength Exercise Protocol | General | Patients | Athletes |
| Contraction Cycle | con/con | con/con | con/ecc |
| Speed/s | 30 up to 180 | 30 up to 180 | 30-300 |
| Trial Repetitions | 0 | 0 | 0 |
| Repetitions | 10 | 10 | 14 |
| Sets | 6 | 6 | up to 12 |
| Rest between sets | 30-60 secs | 30-60 secs | 30 secs |
| Rest between speeds | 2 mins | 2 mins | 2 mins |
| Rest between sides | Nil | Nil | Nil |
| Feedback | bar | bar | bar |
| Endurance Exercise Protocol | General | Patients | Athletes |
| Contraction Cycle | con/con | con/con | con/con |
| Speed/s | 120-180 | 90 | 90-300 |
| Trial Repetitions | 0 | 0 | 0 |
| Repetitions | Max | Max | Max |
| Sets | 1-3 | 1 | 1-3 |
| Rest between sets | 5-10 mins | N/A | 5-10 mins |
| Rest between speeds | 10-30 mins | N/A | 10-30 mins |
| Rest between sides | Nil | Nil | Nil |
| Feedback | bar/pie chart | bar/pie chart | bar/pie chart |
Notes:
Test the uninvolved or dominant limb first.
Stabilisation difficult.
Interpretation:
In the hip it is normal to look at the ratio between the right and left sides there should be a 0-10% difference between the sides. Anything beyond this would indicate a muscle imbalance which would be best corrected.
Eccentric results are generally 30% higher than concentric within the same muscle.
Concentric/concentric ratio; abduction/adduction 0.40% this means the abductors are only 40% of the adductors or the other way around is the adductors are 60% stronger than the abductors.
Hip adductor strain or commonly referred to as a groin strain:
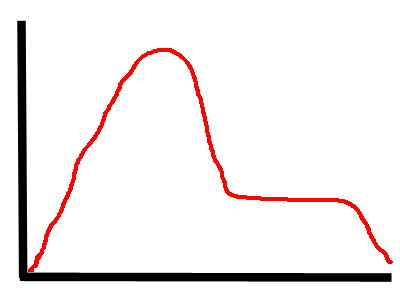
There will often be a large initial curve (due to the elastic build up of tension at the start position of adduction) this will often be followed by a flat portion through range due to neural inhibition.
Normative values:
| Donatelli et al. (1991) | Age | Sex | Machine | ftlbs peak | ftlbs peak |
| speed deg/s | 26 | Abduction | Adduction | ||
| 60 | F | 42.6 | 108.2 | ||
| 60 | M | 63.8 | 152.6 | ||
| Poulmedis et al. (1985) | 28 | M | |||
| 30 | 87.8 | 118 | |||
| 90 | 64.9 | 101 | |||
| 180 | 48.7 | 80.4 | |||
| Tippett (1986) | 20 | M | |||
| 30 dominant | 80 | 104 | |||
| 30 non dominant | 87 | 107 | |||
| Tippett (1986) | 20 | M | |||
| 180 dominant | 48 | 96 | |||
| 180 non dominant | 44 | 97 | |||
| Biodex Values | N/A | Biodex | |||
| abduction/adduction ratio % | Dominantflex/ext% | |
| Donatelli et al (1991) | ||
| 60 | F 26yrs | 0.41 |
| 60 | M 26yrs | 0.48 |
| Poulmedis (1985) | M 28yrs | |
| 30 | 0.74 |
Hip adductor / abductor concentric strength values (based on Cahalan et al 1989 and Donatelli et al 1991)
| Female | Male |
| 18-30 yrs. | 20-40 yrs. | 40-81 yrs. | 18-30 yrs. | 20-40 yrs. | 40-81 yrs. | |
| Adduction | ||||||
| 30/sec | 82 | 63 | 121 | 99 | ||
| 60/sec | 146 | 207 | ||||
| 90/sec | 62 | 44 | 103 | 83 | ||
| Abduction | ||||||
| 30/sec | 66 | 48 | 103 | 75 | ||
| 60/sec | 58 | 86 | ||||
| 90/sec | 54 | 38 | 79 | 63 |