Inversion and Eversion are normally performed in the supine or modified supine (seated) positions.
The ankle poses problems not shared by the knee joint. As it is such a polyarticulating area with a wide variety of movements and allot of muscles spanning it, the ankle throws up many procedural issues, like positioning and alignment, and issues related to closed versus open chain testing.
Inversion and eversion isokinetic tests can be used to evaluate strength properties in many different populations. In recent years it has become very popular in patient groups with recurrent lateral ankle sprains as it is able to detect specific muscle performance deficits. This alows specific treatment to be provided for those individuals. The tests are reliable and intraclass coefficient correlation vary from 0.71 to 0.95. (Pontaga 2004). An isokinetics machine is one of the few ways of reliably testing the ankle to inversions and eversion. Most tests are performed in what is known as the loose packed position (that is the knee is flexed). Testing in the close packed (with the knee straight) position eliminates the influence of the hamstring muscles on tibial torsion. However, this is difficult to replicate but should be used for research. Debate rages over the inclination required at the dynamometer head (i.e. how much it is tilted). Lentell et al. (1988) recommended this be set at 55 degrees.
Supine Lying position:
In this position there is the increased innate thoracic and pelvic stability (little rotation occurs) but the angle of the knee has to be considered. Porter and Kaminski have shown that a knee angle anywhere from 15 to 45 degrees is acceptable for testing. The position of dorsi flexion at the ankle should also be considered. Any angle from neutral to 20 degrees plantar flexion can be used as Zachazewski and Browne (1990) showed no significant change in peak torque when comparing the degree of plantarflexion. Best for research.

To view a set up video see below:
Modified Seated position:
In this position there is even more increased innate thoracic and pelvic stability (little rotation occurs) and the subject is generally more comfortable. The angle of the knee still has to be considered. Porter and Kaminski have shown that a knee angle anywhere from 15 to 45 degrees is acceptable for testing. The position of dorsi flexion at the ankle should also be considered. Any angle from neutral to 20 degrees plantar flexion can be used as Zachazewski and Browne (1990) showed no significant change in peak torque when comparing the degree of plantarflexion. Best for patients.
.

Stabilisation:
Seated: in the seated position stabilisation usually involves holding the bed handles. Most manufacturers supply a thigh / calf stabiliser which can be used to limit knee movement (the knee normally tries to rotate inwards). Whether it is used on the calf or thigh make little difference to the test
Attachments:
The footplate supplied with the machine should fully stabilise the foot it is likley the foot will pull to dorsi flexion during the test so car should be used to full tighten any straps
Axis of rotation:
The axis of rotation goes from the machine and extends through the center of the calcaneous (see below). To check the alignment simply invert and evert the ankle and ensure the heel does not lift from the footplate.

Anatomical zero:
Foot points to roof.
Range of motion:
Inversion and eversion takes place at the subtalar joint. Large individual variations exist in the amount of movement. The ROM should be between 30-50 degrees inversion and 15-20 degrees eversion (Miller, 1995). For eversion between 15-20 degrees is suitable remember not to go too far as the evertors tire very quickly. If you set too large a range of motion the muscles will suffer from muscular inefficiency and the test will stop as the end of range can not be attained. The range of motion for inversion is normally between 30 and 50 degrees (remember these are the values shown on the machine they are not necessarily the true range of motion)
Gravity correction:
The effects of gravity are negligable in this position in fact some manufacturers use a counter balance rather than instrumented correction.
Speeds:
Speeds tend to be lower in the ankle with multiples of 30 being common. However, any speed from 30-240 degrees/second could be considered representative of the speed of subtalar movement during walking/running. A mid range speed for ordinary subjects is 45 degrees per second which will offer good results.
Generally it is accepted that speeds of 30 degrees/second and multiples of this should be used.
Ankle Inversion / Eversion Protocols:
Muscles involved:
Tibialis anterior/posterior and peronei group
| Strength Test Protocols | General | Patients | Athletes | Research |
| Contraction Cycle | con/con | con/con | con/concon/ecc | con/conecc/ecc |
| Speed/s | 45 or 90 | 30 or 45 | 30-300 | 30-500 |
| Trial Repetitions | 0 | 0 | 0 | 3 |
| Repetitions | 10 | 10 | 10 | 5 |
| Sets | 3 | 3 | 4 | up to 9 |
| Rest between sets | 20-30 secs | 20-30 secs | 20-30 secs | 20 secs |
| Rest between speeds | 2 minutes | 2 minutes | 2 minutes | 2-5 minutes |
| Rest between sides | 5 minutes | 5 minutes | 5 minutes | 5 minutes |
| Feedback | nil | nil | nil | nil |
| Endurance Test Protocols | General | Patients | Athletes | Research |
| Contraction Cycle | con/con | con/con | con/concon/ecc | con/conecc/ecc |
| Speed/s | 90 | 90 | 90-300 | 90-500 |
| Trial Repetitions | 0 | 0 | 0 | 0 |
| Repetitions | Max | Max | Max | Max |
| Sets | 1 | 1 | 1 | 1 |
| Rest between sets | N\A | N/A | N/A | N/A |
| Rest between speeds | 10-15 mins | 10-15 mins | 10-15 mins | 10-30 mins |
| Rest between sides | 5 mins | 5 mins | 5 mins | 5 mins |
| Feedback | nil | nil | nil | nil |
| Strength Exercise Protocol | General | Patients | Athletes |
| Contraction Cycle | con/con | con/con | con/ecc |
| Speed/s | 60 up to 180 | 45 up to 180 | 30-300 |
| Trial Repetitions | 0 | 0 | 0 |
| Repetitions | 10 | 10 | 14 |
| Sets | 6 | 6 | up to 12 |
| Rest between sets | 30-60 secs | 30-60 secs | 30 secs |
| Rest between speeds | 2 mins | 2 mins | 2 mins |
| Rest between sides | Nil | Nil | Nil |
| Feedback | bar | bar | bar |
| Endurance Exercise Protocol | General | Patients | Athletes |
| Contraction Cycle | con/con | con/con | con/con |
| Speed/s | 90-180 | 90-180 | 90-300 |
| Trial Repetitions | 0 | 0 | 0 |
| Repetitions | Max | Max | Max |
| Sets | 1-3 | 1 | 1-3 |
| Rest between sets | 5-10 mins | N/A | 5-10 mins |
| Rest between speeds | 10-30 mins | N/A | 10-30 mins |
| Rest between sides | Nil | Nil | Nil |
| Feedback | bar/pie chart | bar/pie chart | bar/pie chart |
Notes:
Test the uninvolved or dominant limb first.
Interpretation:
In the ankle it is normal to look at the ratio between the right and left sides there should be a 0-10% difference between the sides. Anything beyond this would indicate a muscle imbalance which would be best corrected.
Eccentric results are generally 30% higher than concentric within the same muscle. In pathology of the lateral ankle complex the eccentric results can be drastically reduced. Restoration of this imbalance is crucial.
Concentric/concentric: Inversion/eversion ratio should show a invertor dominance of 30 percent.
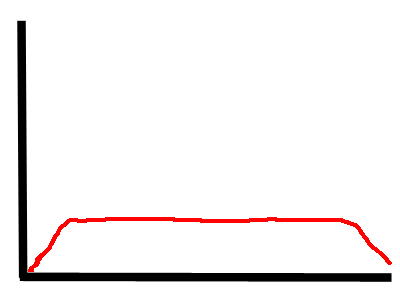
Anterior Talo Fibular Ligament (ATFL) sprain/strain:
When the ATFL is disrupted it has an inhibitory effect on the peronei muscles. This leads to a lack of peak in the torque curve of the evertors giving a flat mid portion. The effect is seen first in the eccentric results then at it’s worst in the concentric results.
Normative values:
| Davies (1992) | Age | Sex | Machine | PTBW | PTBW |
| speed deg/s | Cybex | Inversion | Eversion | ||
| 60 | 12 | 11 | |||
| 120 | 10 | 9 | |||
| Biodex Values | M | PTBW | PTBW | ||
| 30 | 12-16 | 13-17 | |||
| 60 | 11-14 | 9-12 | |||
| F | |||||
| 30 | 14-19 | 12-16 | |||
| 60 | 12-15 | 9-12 |
Values for invertor and evertor group concentric and eccentric strength (in Nm). Based on Ivey et al (1985), Cahalan et al (1991) and + Shkiar & Dvir (1994) sedentary subjects.
| Female | Male |
| Age | 19-30 | 30-40 | 40-50 | 50-62 | 19-30 | 30-40 | 40-50 | 50-62 |
| Invertors | ||||||||
| 60/sec | 23 | 25 | 18 | 20 | 36 | 31 | 29 | 30 |
| 120/sec | 20 | 21 | 18 | 17 | 32 | 26 | 25 | 23 |
| Evertors | ||||||||
| 60/sec | 20 | 18 | 20 | 16 | 29 | 25 | 25 | 24 |
| 120/sec | 16 | 14 | 13 | 13 | 23 | 19 | 18 | 18 |